I sat astride his chest, ‘It’s just a thrill,’ he said,
As he relaxed on the dark, dark bed, ‘it’s just breath control.’
He whispered ‘Hold me here’ and I did and his head fell back.
He whispered ‘Press harder’ and I did and his eyes rolled back.
It’s just breath control. Just breath control.Read more: Recoil – Breath Control Lyrics | MetroLyrics
One of the insights I had into the overall historical arc of BDSM is the issue of safety, who decides what is safe, and how, and how is that knowledge distributed. My thoughts on this crystallized after a recent weekend workshop on rough play, which included a discussion on edgeplay and the risks involved in thinks like choking and other forms of breathplay.
Some of the legal discourse about BDSM, notably in the Operation Spanner case, has compared BDSM to sports, in terms of consensual activities with a risk of injury or death. Historically, pursuits like boxing, wrestling, gridiron football, etc, have gone through a process of “taming”, with the developments of rules that specify required protective gear, proscribed conduct in play, and the like.
Football’s distant ancestor, medieval football, was a social ritual just shy of a riot, in which unlimited number of people from two villages would try to move an inflated pig’s bladder to markers at either end of town, using any means available short of manslaughter or murder. This kind of quasi-sport mostly ended with the Highway Act of 1835 banned football on public highways. [Source]
American football, which evolved from rugby and association football, broke with its ancestors by allowing contact interference, i.e. blocking.
Despite these new rules, football remained a violent sport. Dangerous mass-formations, which involved interlocking interference, like the flying wedge resulted in serious injuries and deaths. A 1905 peak of 19 fatalities nationwide resulted in a threat by President Theodore Roosevelt to abolish the game unless major changes were made. [Note: this article disputes this claim.] In response, sixty-two colleges and universities met in New York City to discuss rule changes on December 28, 1905, and these proceedings resulted in the formation of the Intercollegiate Athletic Association of the United States, later named the National Collegiate Athletic Association (NCAA). [Wikipedia]
Through the early 20th century, the rules of football were formalized and revised in the hopes of reducing injuries. Helmets became mandatory in college football in 1939 and in professional football in 1943.
Boxing went through a similar process. The Queensbury rules, published in 1867, were one of a series of versions of rules to regulate boxing. They were the first to make boxing gloves mandatory and forbid bare-knuckle boxing, which could last for hours.
This process is obviously still ongoing, with the controversies about the long-term impacts on the mental and physical health of boxers, football players and other athletes in contact sports.
BDSM has gone through a similar process of taming. While people have been doing erotic flagellation for a long, long time, it’s only relatively recently that it has accumulated a body of knowledge of how to do it safely and effectively. I would guess that sex workers who providing erotic flagellation in the 18th and 19th centuries evolved some kind of practical knowledge about it, though I doubt it was effectively spread. We know that the leatherman culture of the 50s and 60s had an apprenticeship-like system for spreading knowledge. It wasn’t until the early 1970s, with the launch of TES and SOJ, that we saw the beginnings of workshops and more formal systems of education.
Whereas boxing, football and other contact sports have gone a public, formalized process, influenced by medical, scientific and legal discourses, BDSM practices have remained largely subcultural, a “folk knowledge”.
Sarah Thornton (1996) uses the term ‘subcultural capital’ to refer to the knowledge, dispositions and practices that are rewarded with recognition and admiration within subcultures. According to Thornton, this subcultural capital is used by subculture participants to assert their distinction from commercial mass culture. Being ‘in the know’ is certainly valued within the Undercroft community, with the skaters we interviewed demonstrating in-depth collective knowledge of the histories and practices associated with the space. Whilst this knowledge represents capital in Thornton’s terms, this knowledge was shared across groups and generations rather than protected to assert individual power. [source]
It has evolved haphazardly through practitioners sharing knowledge, not through a formalized system of experts, research and review. To my knowledge, there are no organizations scientifically studying the health risks of BDSM play, the way the Food and Drug Administration studies the impact of diet or medicine. There are no appeals to credentialed experts or institutions seen as reliable. Each kinky person must make their own decision about which practices are safe enough for them, in the absence of the usual sources of medical knowledge.
The big problem is that human beings, generally speaking, are not very good at assessing and comparing risk. Witness webcomic xkcd:
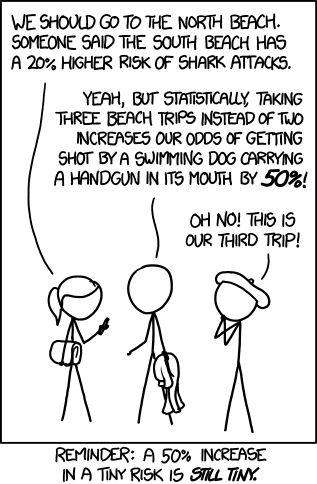
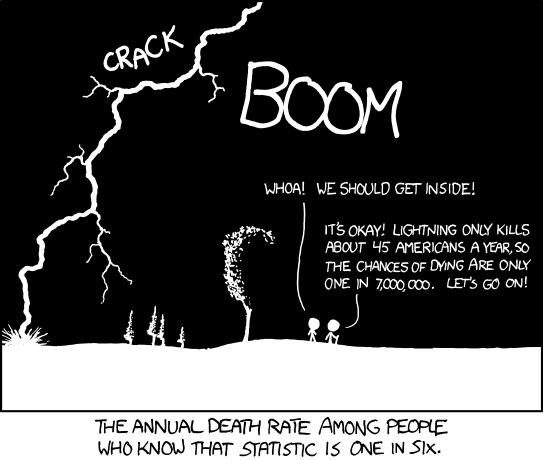
We have an inordinate fear of things that are highly unlikely to kill us, such as terrorist attacks or predation by wild animals, and are blasé about everyday risks like smoking tobacco, drinking alcohol, or bad driving habits. Cows kill more people than sharks every year. [source] I can recall a time in the 90s when there was concern that a person could contract HIV or hepatitis by being near an infected person being flogged and inhaling the bottom’s aerosolized blood. According to the CDC:
Although it is known that bloodborne pathogens can be transmitted through mucous membrane exposure, there are no known instances of a bloodborne pathogen being transmitted by an aerosol in a clinical setting. […] The possibility that HIV may be transmitted via aerosolized blood must be considered theoretical at this time.
Is contracting HIV from being near a whipping or knifeplay scene a realistic possibility, or are you more likely to die in a car accident on the way home from the club?
This ties into the evolving philosophies of BDSM, from SSC (“Safe Sane and Consensual”) to RACK (“Risk Aware Consensual Kink”) to PRICK (“Personally Responsible, Informed Consensual Kink”). As I see it, the difference between SSC and RACK is not about the acts themselves, but the attitudes towards risk. SSC implicitly argued that you could divide BDSM play into “safe” and “not safe”, the latter including activities like cutting and breathplay. RACK says that is a fallacy. Nothing is absolutely safe, and what activity has an acceptable degree of safety varies with the particular situation and the people involved.
I still retain the belief that breathplay is the epitome of edgeplay, the unacceptable risk, the invitation to death, veering close to dark tales of people found dead from autoerotic asphyxiation. That belief, I will admit, is not founded on anything like a rational assessment of the dangers. Just exactly how dangerous is it?
Jay Wiseman, a BDSM author (notably of SM 101: A Realistic Introduction) and educator, and a former Emergency Medical Technician (ambulance medic), has been involved in this particular issue for many years. In SM 101 (published 1992), he wrote:
Choking, suffocation, and other forms of “breath control” are sometimes played with. Among other things, the first symptom of oxygen deprivation is often euphoria. […] Unfortunately, this area is the single most dangerous aspect of SM-related play.
After a great deal of investigation, consideration, and discussing this subject with people who have much more medical knowledge than I have, I have been completely unable to learn any way to make breath control acceptably safe. Furthermore, the overwhelming majority of SM-related fatalities I have heard of were related somehow to restricting breathing.
Wiseman also wrote about breathplay back in the USENET days, when the newsgroup soc.subculture.bondage-bdsm was a major hub of the English-speaking kinky world.
In a 1996 post, he wrote:
As has been prominently pointed out, in my latest post regarding the risks of breath control play I mentioned a concern that I had not raised in my previous posts: That there is hypoxia-induced _cumulative_ brain damage associated with strangulation and/or suffocation even if no major primary complication, such as cardiac arrest, or secondary complication, such as a seizure, occurs. Several people, understandably, asked me how I “really knew” that cumulative damage took place.
Well, truth be told, I didn’t, directly, know that it was true. I *did* have pretty good reason to believe that it was true. After all, two M.D. Neurologists and a PhD Neurophysiologist had told me that cumulative damage occurred. Also, another SM friend had told me that he had been told by an Anesthesiologist that it occurred. So I had been advised, either directly or indirectly, by no fewer than four people with extensive professional training in how the nervous system functioned that cumulative damage occurred secondary to episodes of cerebral hypo-oxygenation.
Note that Wiseman refers to what are basically anecdotes, though coming from medical experts, not medical or scientific studies. He acknowledges that this was a flaw.
Still, the requests for documentation were not unreasonable, and I can see a world-class medical school from my bedroom window, so I got myself over to its library and spent the better part of a day searching for verifiable, scientific-quality, information to support or (God forbid!) refute my claim.
He then cites three journal articles about the effect of oxygen deprivation on the brain.
Here’s another essay he posted, copyrighted 1997:
For some time now, I have felt that the practices of suffocation and/or strangulation done in an erotic context (generically known as breath control play; more properly known as asphyxiophilia) were in fact far more dangerous than they are generally perceived to be. As a person with years of medical education and experience, I know of no way whatsoever that either suffocation or strangulation can be done in a way that does not intrinsically put the recipient at risk of cardiac arrest. (There are also numerous additional risks; more on them later.) Furthermore, and my *biggest* concern, I know of no reliable way to determine when such a cardiac arrest has become imminent.
[…]
I have discussed my concerns regarding breath control with well over a dozen SM-positive physicians, and with numerous other SM-positive health professionals, and all share my concerns. We have discussed how breath control might be done in a way that is not life-threatening, and come up blank. We have discussed how the risk might be significantly reduced, and come up blank. We have discussed how it might be determined that an arrest is imminent, and come up blank.
Indeed, so far not one (repeat, not one) single physician, nurse, paramedic, chiropractor, physiologist, or other person with substantial training in how a human body works has been willing to step forth and teach a form of breath control play that they are willing to assert is acceptably safe — i.e., does not put the recipient at imminent, unpredictable risk of dying. I believe this fact makes a major statement.
Wiseman couches his argument in medical discourse, by citing his own medical credentials as well of those of the people he consulted. He was using the two main channels available for distribution of BDSM information: published books and online networks like alt.sex.bondage and soc.subculture.bdsm-bondage. The latter probably had the greater reach in terms of people.
Later, Wiseman wrote a 2010 essay of over 27,000 words on the subject, from medical and legal perspectives. This also discusses in depth the ideas of “harm reduction” by teaching people how to do breathplay as safely as possible, versus blanket condemnation (a debate similar to the terms regarding mind-altering substances). He’s so thoroughly permeated the idea-space that it’s hard to find a mention of breathplay that doesn’t link to his writings.
(Margot Weiss’ book Techniques of Pleasure also covers this issue.)
Wiseman’s argument would seem to be pretty final, but there are questions of exactly how to define breathplay. This blog post by Maxine from 2010 cites Wiseman’s research, but it also talks about several activities that can be classified as breathplay, but are not about depriving the brain of oxygen. [Emphasis in original]
However… there are things that I would class as ‘breath play’ which Mr Wiseman doesn’t talk about, and I would consider to be relatively safe, even having read and fully understood these warnings.
Maxine discusses things like “Breath exercises such as one might do with a singing teacher” and “Tantric breath exercises such as ‘circular breathing'”, and “Kissing and instructing a partner to ‘breathe through you'”. She also specifies “Things I will NOT do, as a top:“, such as:
I will not perform any sort of breath play where my partner cannot pull back and control their own breathing – no gas masks, no bags, no cling film, no masks without airholes, and if a hand goes over a mouth it will be loosely so that my partner can breathe normally when they need to.
I will not put pressure on the neck in such a way that either the windpipe, or the major arteries to the brain will be affected (in other words, I will not put pressure on the neck).
I will not put myself, or my partners knowingly at risk of brain damage or heart attack.
While Wiseman and Maxine are in dialogue about the dangers of “breathplay”, they’re using different definitions of the same term. Wiseman’s medicalized discourse focuses on the effects of oxygen deprivation on the brain, while Maxine’s discourse, borrowing from less clinical sources such as arts and meditation, includes a broader range of activities, and draws her own line between acceptable and unacceptable risks in breathplay. Note that Wiseman is making categorical statements about breathplay, while Maxine only writes about her own self-imposed limits. There’s no central authority they can refer to about what exactly breathplay is, nor does Wiseman have any particular authority to impose his arguments other than persuasion.
In part, BDSM’s subcultural discourse has been in opposition the medical-psychiatric discourse of sexual deviance. It’s knowledge that evolved from the practical experiences of many diverse practitioners, bottom-up (so to speak). Wiseman is going against the grain by arguing as a medical expert and positioning himself as the go-to expert on breathplay.
There’s a further complication in that while Wiseman is speaking from within the BDSM community, choking and other forms of breathplay are found under the nebulous discourse of “rough sex”, which functions outside the BDSM culture, and has no experts, self-appointed or not. We know of many examples of people who have died from autoerotic asphyxiation, and children or teenagers who play the “choking game”. Referring back to the parallels about drugs, how can you control a “drug” that any person can “make” with their own body?
The “taming” of BDSM has come a long way in the past 30 years or so, but there are still edges to the process. Humans still have a need to seek the extremes of experience, despite the risks involved. Wiseman’s self-appointed task is admirable, but could also be seen as ultimately futile.
William Blake wrote in Proverbs of Hell that, “You cannot know what is enough until you know what is more than enough.” Michael Jackson wrote, in “Dirty Diana”, “I want to go too far.” Some people will always want to go too far.
Further reading:
- Kinsey Confidential’s article on breathplay
- Another personal blog post about safer alternatives to oxygen-deprivation breathplay
- Video interview with Jay Wiseman
- Satirical article about Wiseman reversing his position
Addendum: Lisa Downing’s essay “Beyond Safety: Erotic Asphyxiation and the Limits of SM discourse” (in Langdridge, Darren, and Meg Barker. 2007. Safe, sane, and consensual: contemporary perspectives on sadomasochism. Houndmills, Basingstoke, Hampshire [England]: Palgrave Macmillan) discusses many of the same points, and asks if BDSM educators are engaging in a kind of “respectability politics” by drawing a line between life-affirming BDSM and overly dangerous, high risk breath play and other activities.